Day Zero of My Posture Experiment: X-Ray, Diagnosis, and the Plan

I train 5-6 times a week. HIIT twice. Futsal 3-4 times. I'm not lazy.
My posture is still terrible.
If you sit at a desk for 8 hours a day, all the evening training in the world won't save you. I've been running that experiment on my own body for 10 years. The result is in: the desk wins.
So I'm starting a different experiment. Short daily mobility work, done during the workday, for as long as it takes. 5 minutes a day. 3 micro-breaks (2 min, 2 min, 1 min). Public log. I'll document it all, including the days I skip. And if nothing good comes out of it, I'll publish that too.
TL;DR
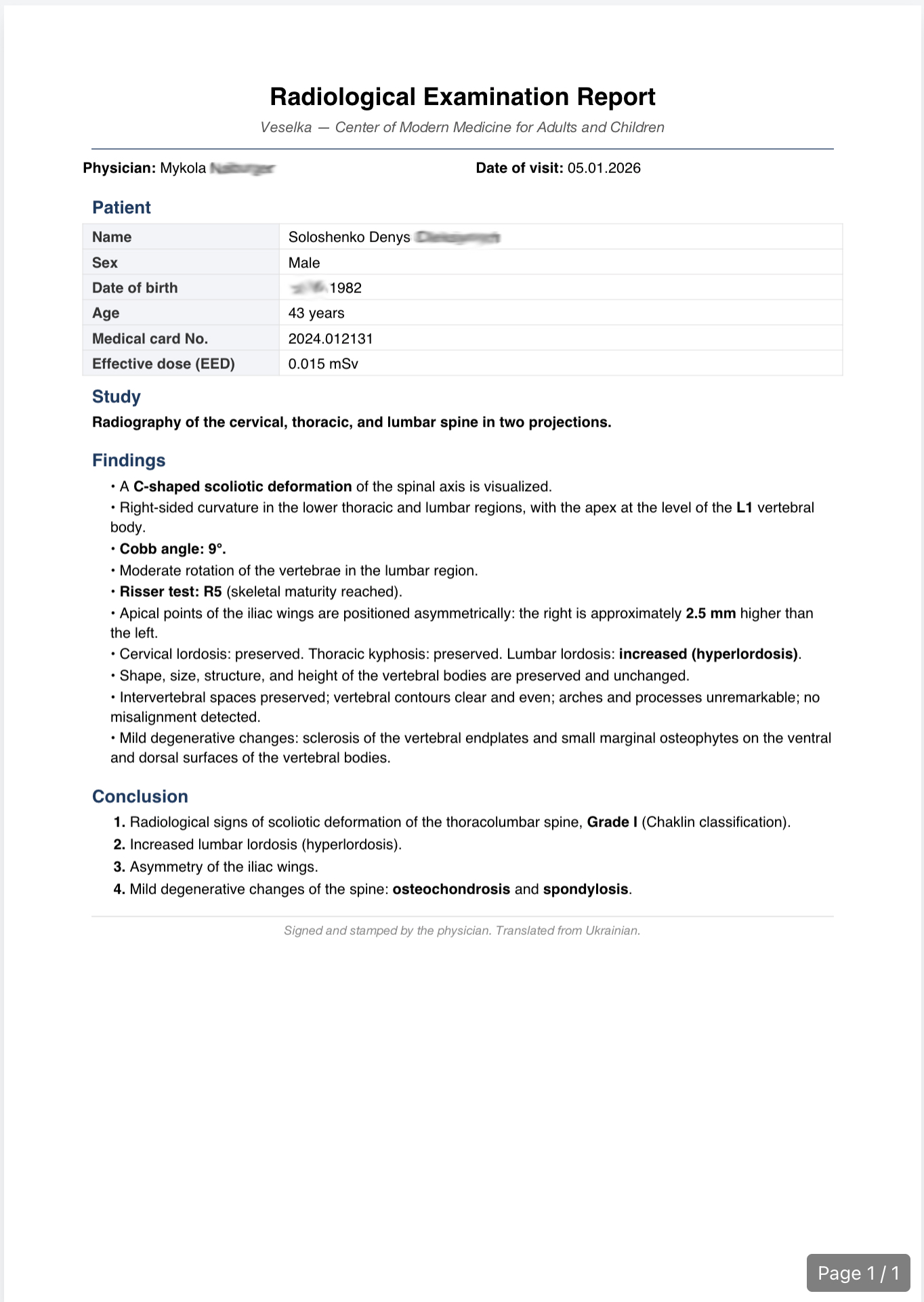
I'm 43, a developer. Two doctors looked at my X-ray. I have mild scoliosis (a sideways curve of the spine, 8-9°), increased lumbar lordosis (an overly arched lower back), mild osteochondrosis (wear on the discs between the vertebrae), and mild spondylosis (age-related wear of the spine, often with small bony outgrowths). No surgery. Two of those diagnoses cannot be reversed. I picked 18 mobility and posture exercises, all of which have peer-reviewed support for this kind of work. The dose: 5 minutes a day, 3 short breaks during the workday. Real measurement re-check at day 30, 60, and 90. Short qualitative check-ins every 2 weeks. Day-by-day log lives 📓 here.

Medical disclaimer (read this first)
I'm not a doctor. Not a physiotherapist. Not a coach. I'm a developer experimenting on himself after getting his own spine imaged and checked by two clinicians. Nothing in this post is medical advice. If you have back pain, a known spinal condition, or anything else going on, talk to a qualified clinician before copying what I'm doing. Your spine is not my spine.
Where I cite a study, the link is in-line and goes to the original source (mostly PubMed or PMC).
Table of contents
- Who I am
- Why I'm doing this
- What I actually want (the goal)
- The doctor visit and the X-ray
- At-home assessment (Day Zero baselines)
- The 18 exercises, with research behind each
- The whole plan
- What I'm asking from you
- What the research actually says (overall)
- FAQ
1. Who I am
Denys. 43. Developer with 25+ years of shipping code for a living. Still playing amateur futsal with guys younger than me. HIIT twice a week with a coach. Not the couch type.
I'm building 1 Pixel Workout, a browser extension that intercepts your doomscroll and swaps it for a 60-second desk workout. The whole idea is to make fitness feel automatic instead of optional. Or as I put it in my head: make fitness addictive. I am not there yet. The product is early, I skip workouts myself, and the only way I can tell if the thing actually works is to run it on myself in public.
This posture experiment is that run. I built 1 Pixel Workout for exercise snacks, and now I'm adapting the same tool to fix my own spine.
The deeper context, if you care: I was an extremely shy kid. Walking into a room, I tried to become small. Shoulders forward, head down. That's 15 years of dealing with it compounded on top of another 25 years at a keyboard. The body remembers.
2. Why I'm doing this
I hate how I look on camera. Photos, video calls, recordings for my project. I see the rounded shoulders, the forward head (the dev Reddit crowd calls it "nerd neck"), and I close the tab.
Breathing is harder than it used to be. This is the one that actually scares me. My ribcage doesn't open the way it did in my 30s. I feel my upper back pressing on my lungs when I try a full inhale. Not dangerous yet. Also not a direction I want to keep going.
My two-year-old daughter started copying my posture. That one hit different. You can ignore your photos for 20 years. You can't watch your kid copy how you sit.
The X-ray came back with news I did not want. More on that in section 4.
If you've ever opened a side-profile photo of yourself and immediately closed it, we have the same problem.
3. What I actually want
I don't want to look like a fitness influencer in a Reel.
What I want:
- Unlock my spine. Specifically the thoracic. Reach overhead without my upper back fighting me.
- Build an actual stretching habit. I fail at yoga after three days. Every time. 1 Pixel Workout exists because I needed a way to move that didn't feel like a separate appointment on my calendar.
- Slow down the things I can't reverse. Osteochondrosis and spondylosis don't undo. They also don't have to get worse on a straight line. Every month I move well is a month I bought back.
- Move better at futsal matches. Hip mobility, thoracic rotation, ankle range. Those separate "still playing at 43" from "watching from the sideline."
- Be able to learn surfing some day without falling apart.
And if I stop cringing at my own side profile, I'll take that too.
4. The doctor visit and the X-ray
In January I went to two clinics. First an X-ray clinic for the image and their reading. Then the Institute of the Spine, a rehab clinic that specializes in spinal conditions. I wanted two independent reads before committing to a plan.


The good news
No surgery. I asked first. Both doctors said no. I was genuinely scared about this one.
The expected news
Scoliosis, 8-9 degrees on the Cobb angle. The Cobb angle (the degree of sideways curve measured on an X-ray) is how doctors grade scoliosis. Under 10° is the threshold where non-surgical management is standard. I'm under the line.
Increased lumbar lordosis. My lower back arches more than it should. It's trying to balance out whatever is happening above it. In my case, 25 years of hunching over a laptop.
Forward head posture (the head drifting in front of the shoulders, measured at home rather than on the X-ray). My tragus sits 15 cm in front of the wall when I stand naturally. Normal is close to zero. Developers call it "nerd neck." It's also the one I can probably change the fastest with exercise. See section 6, exercise #2 (chin tuck), which has Level 1a evidence behind it.
The bad news
Two diagnoses I wasn't ready for.
Osteochondrosis (mild). The discs between my vertebrae are drying out. They lose water, lose elasticity, and start acting more like bone than like shock absorbers. When I hear "osteochondrosis" I think of someone in their 70s. My doctor said "normal for your age." I hate hearing "for your age." It's a polite way of saying "you're old, get used to it."
Spondylosis (mild). The spine grows extra bone around itself as a stability response. It's the body duct-taping itself.
The part that got to me: both are irreversible. I can't undo them. I can only slow them down. The goal from here is to stay functional for as long as possible.
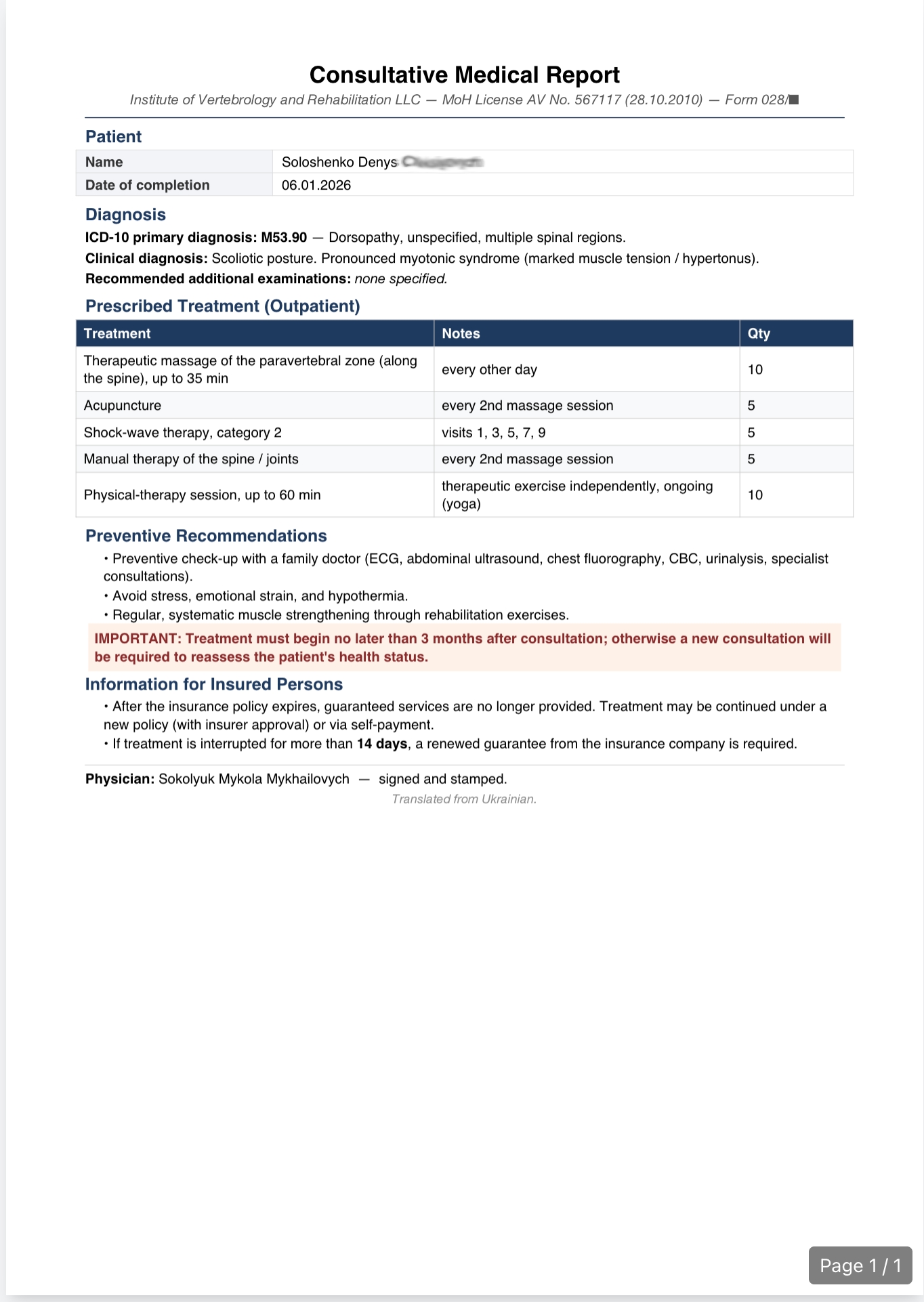
What the doctors recommended
- Massage for chronic spinal muscle tension
- Dry needling (needle therapy)
- Yoga or structured mobility work
This post covers the mobility work. I can't really afford regular massage (both time and money), so I'll use foam rolling for now and see if it helps at least a bit. If massage and needling turn out to matter, I'll write about them in the journal.
Get an X-ray. Seriously.
I had no back pain. None. Not even a little. I'd have bet money my spine was fine. It was not.
If you're in your 30s or 40s, you sit at a desk all day, and you've never had a spinal X-ray, go get one. Pain is a late signal. By the time it shows up, things have been trending in the wrong direction for years.
5. At-home assessment (Day Zero baselines)
I'm not going to X-ray myself every month. Too expensive. Too much radiation. I needed cheap, repeatable measurements I can do alone with a tape measure and a wall.
None of these are clinically validated. They're just consistent enough to track change. If you know better ones, leave a comment on the video.
Measurement 1: side-profile photo
Same wall. Same lighting. Same bare feet. One shot relaxed. One standing as straight as I can manage. Retake every 30 days, stack side by side.
Visual progress is the most motivating kind, especially for an ADHD brain that forgets why it started.



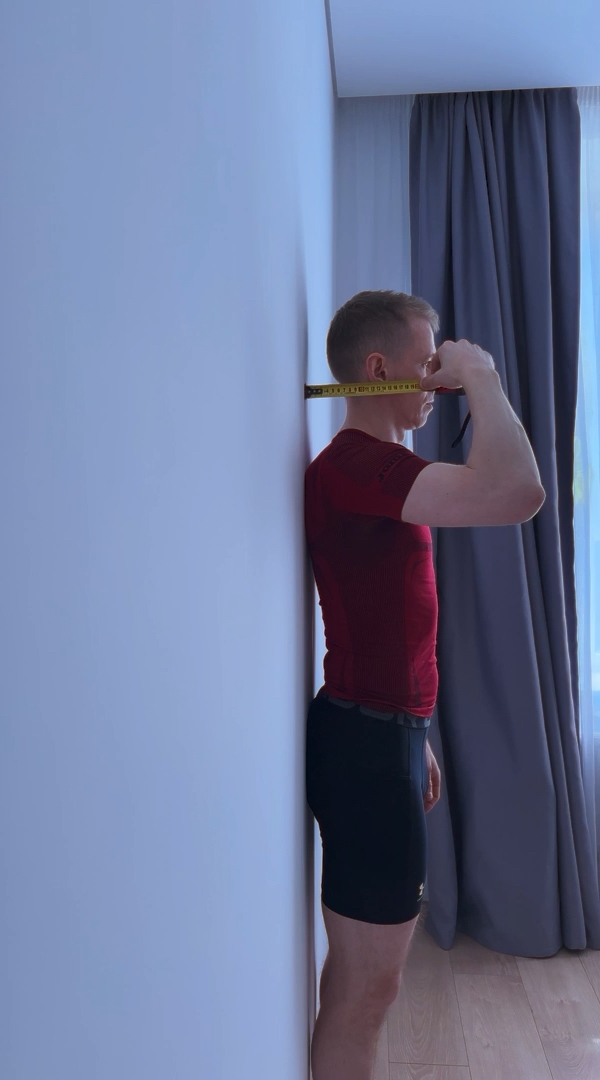
Measurement 2: tragus-to-wall distance (forward head test)
Heels, glutes, and upper back flat against the wall. Head stays in its natural resting position. I don't force it back. Measure the distance from the wall to the tragus (the small cartilage bump in front of the ear canal).
This one is tricky. It highly depends on how much I relaxed and change the number by a couple of centimeters. 15 cm is when I'm not too much relaxed, trying a bit to stay straight. Hard to say actually how to do this one properly.
Measurement 3: overhead floor reach (shoulder + thoracic mobility)
Thoracic mobility (how well the mid-back rotates and extends) tends to be the first thing to go in desk workers.
Lie on the floor. Knees bent. Lower back flat against the floor. Arms overhead with elbows locked straight. Measure the distance between the back of my hands and the floor.
Day Zero number: about 28-30 cm off the floor, and my lower back was still trying to arch to cheat. Brutal. Expected bad. Got worse than bad.

Measurement 4: cow face pose shoulder test
One hand over the shoulder reaching down the back. The other hand up the back from below. Try to touch fingers.


Clear asymmetry.
Day Zero tracking table
| # | Measurement | Day 0 | Day 30 | Day 60 | Day 90 |
|---|---|---|---|---|---|
| 1 | Side-profile photo | [photo saved] | |||
| 2 | Tragus-to-wall (avg of 3) | 15 cm | |||
| 3 | Overhead floor reach | ~28-30 cm | |||
| 4 | Cow face (bad side) | Fingers barely touch (one side) |
Numbers get redone every 30 days. In between, every 2 weeks, I'll post a short qualitative check-in in the journal: how it feels, what's easier, what still sucks. The hard numbers are the honest part. If something goes in the wrong direction, it goes in the wrong direction. No cherry-picking.
6. The 18 exercises, with research behind each
I'm not inventing anything. These are standard mobility and postural exercises. I picked them because they map to what the X-ray and the home tests flagged: tight thoracic spine, forward head, internally rotated shoulders, tight hip flexors, limited overhead range, and clear left/right shoulder asymmetry.
Why this batch? Two reasons. First, I did the research on every move I'd heard recommended and kept only the ones with real evidence (more on that in section 9). Second, and just as important: every single one can be done with a wall, a floor, or a doorframe. No gym. No bands. No foam roller required. I need it to survive a normal workday, not a weekend retreat.
Before the list, one thing worth knowing. A 2024 meta-analysis of 23 studies covering 969 healthy participants (Warneke, Lohmann & Wilke, Sports Med Open) found that chronic strengthening changed posture with a large effect (d = -0.83, P = 0.01), while chronic stretching alone didn't (d = -0.19, P = 0.16). When the authors compared the two head-to-head, strengthening won (d = 0.81, P = 0.004). The effect was concentrated where it matters most for desk-worker posture: in the thoracic and cervical spine, strengthening produced an even larger effect (d = -1.04, P = 0.005). The stretches on this list are on it for good reasons: they restore range of motion, reduce pain, and prep the body for the strengthening work. But the actual postural change most likely comes from the strengthening: wall angels, chin tucks, prone YTW raises, and external rotation. That's the hypothesis I'm testing on myself over 30 days.
Upper back and posture reset
1. Wall angels. Stand with your back against the wall, arms in a "goalpost" shape, slide them overhead while keeping elbows, wrists, and back flat. The most painful one for me. You saw me fail it in the assessment video.
Research. EMG study by Hardwick et al., 2006 (JOSPT) confirmed wall slides effectively activate the serratus anterior, especially above 90°. A 2025 trial in Journal of Sport Rehabilitation found scapular upward rotation improved 5.4° immediately and 7.6° after 2 weeks (8 reps × 3 sets, 6 sessions). Kim & Lim, 2016 showed significant improvement in radiographic scapular alignment after 4 weeks of wall slides.
2. Chin tuck. Pull the head straight back over the shoulders. Like making a deliberate double chin. Deceptively simple, embarrassingly hard after a decade of leading with the face.
Research. Chin tuck (also called cervical retraction) is probably the most-prescribed exercise for forward head posture, so I went digging to see if that's actually backed by evidence or just folklore. It's a bit messier than I hoped. A meta-analysis of 7 RCTs with 627 participants (Sheikhhoseini et al., 2018) found Level 1a evidence that corrective exercises change the craniovertebral angle (OR = 6.7, P = .0005), but those trials mixed several exercises in each protocol. So I can't say chin tuck alone did the work. A more direct study on 43 people with FHP (Sureshbabu et al., 2021) tested chin tucks on their own and saw a significant CVA improvement (P = 0.0001), though it was small and short-term. Biomechanical modeling (Han et al., 2018) also shows chin tuck reduces the abnormal joint forces in FHP necks. At least the mechanism is sound. Not airtight, but enough for me to keep it in.
Neck
3. Neck lateral stretches. Ear to shoulder, hold, switch. Nothing fancy.
4. Neck flexion-extension (look up, look down). Full range, slow. My doctor said my neck range could be better. I'm literally practicing the basics.
5. Head side to side (cervical rotation). Same idea, sideways.
Research. I couldn't find studies that isolated any one of these three movements, which makes sense. Nobody runs a trial on "ear to shoulder alone." What's been tested is general neck mobility and stretching programs that include these as components. A 4-week RCT on 96 office workers with chronic neck pain (Tunwattanapong et al., 2015) found a neck and shoulder stretching program done 2×/day significantly reduced pain and improved neck function. A longer 12-month RCT on 180 female office workers (Ylinen et al., 2010) showed the "stretching-only" group still cut their cervicogenic headache by 37% at follow-up. Honest read: stretching alone helps, but it's the weakest of the three arms in that study. The groups that added strength or endurance training got up to 69% reduction. For rotation specifically, Röijezon et al., 2010 showed women with chronic neck pain rotate their heads noticeably slower than healthy controls (226°/s vs. 348°/s peak speed). That's not intervention evidence and it doesn't prove the exercise fixes anything, but rotation speed is a real, measurable marker of a healthy neck. Good enough reason to keep these in as a daily warm-up, low time cost, low risk.
Shoulders
6. Seated shoulder external rotation. Elbow tucked to the ribs, forearm rotates out. Opposes the inward rotation from typing all day.
Research. This is the strongest shoulder exercise on the list by evidence quality. Reinold et al., 2004, in a well-cited JOSPT EMG study, quantified 7 different external rotation positions and showed that ER exercises strongly activate the infraspinatus and teres minor, the rotator cuff muscles you want firing to counter internal-rotation dominance from desk work. (Sidelying ER scored best for isolating those muscles; seated ER is still effective, just less targeted.) A systematic review by Schory et al., 2016 found ER with the elbow at 90° gives favorable middle trapezius activation without the upper trap taking over. That's the exact pattern you want for undoing upper crossed syndrome (tight chest and upper traps, weak deep neck flexors and mid-back).
7. Chicken wing elbow circles. Hands on shoulders, draw big circles with the elbows, forward then backward. Wakes up the whole shoulder joint. Actually, I think it's rather warm up than some real posture correction exercise. But I'll keep it at least for 2 weeks. Then decide.
8. Wall lat stretch. Forearms on the wall, hips back, chest drops. Opens the lats.
9. Desk lat stretch. Same idea as #8 but done at a desk. Survives the "I can't leave my chair" excuse.
10. Cow face pose. One arm overhead, one behind the back, try to touch. Stretches both shoulders in opposite directions at once. I'm doing extra reps on my restricted side.
11. Butcher block stretch. Kneel, forearms on an elevated surface (bench, coffee table), chest drops toward the floor. Deep shoulder and lat opener.
Research. I'll be honest: none of these five mobility drills has its own clean RCT. What's been tested is programs that include this kind of movement as a component. A systematic review of workplace exercise interventions (Tersa-Miralles et al., 2022) concluded that workplace exercise — including stretching and mobility work — reduces neck, shoulder, and back pain in office workers. A 12-week controlled study of ~350 office workers (Holzgreve et al., 2021) found 10 minutes of stretching, twice a week, produced measurable gains in range of motion and reductions in musculoskeletal complaints. For the lat stretches specifically, Herrington & Horsley (2013) showed that short lats directly restrict shoulder flexion. Stretching them is mechanistically defensible, even if nobody's run a trial on "wall lat stretch" by name. Good enough for me to keep these in as low-cost, low-risk opens for typing-compressed shoulders, but I'm not going to oversell them.
Chest
12. Doorway (or corner) pec stretch. Forearm on the doorframe, step through, rotate away. Opens the chest that's been shortened by years of hunching.
Research. Decent evidence, but I had to dig past a lot of hype. The most direct study is on 34 high-school baseball players who did a single doorway stretch (Higuchi et al., 2021). Pectoralis minor length and glenohumeral internal rotation ROM both increased significantly (P < .01), and the scapula shifted into a more posteriorly-tilted resting position. One session, same day. Different population from desk workers, but the mechanism is what I care about. Longer-term, a blinded RCT on 28 adults (Wong et al., 2010) combined manual release of pec minor with self-stretching and saw rounded-shoulder posture still significantly reduced 2 weeks later (P < .01 vs placebo), though I can't separate the self-stretch from the manual work they added on top. A 3-week RCT on 60 women (Hasan et al., 2023) suggested pec minor stretching plus lower-trap strengthening beat stretching alone for pec minor length, but not for shoulder flexion ROM. The pattern is "stretch the front, strengthen the back," not "stretching alone fixes it."
Thoracic spine and full spine
13. Wall thoracic extension stretch. Forearms on the wall higher than the head, chest drops. Opens the locked-up middle back.
Research. The landmark RCT is the SHEAF trial (Katzman et al., 2017): 99 older adults with hyperkyphosis, 6 months of targeted spine-strengthening and postural training, primary outcome was radiographic Cobb angle. They got −3.3° vs −0.3° in controls. Modest but real, and it's one of the first RCTs to show exercise changes the actual radiograph, not just a clinical proxy. Closer to desk-worker reality: a 6-week RCT on 32 office workers with forward head posture (Kang, Im, Kim, 2021) tested scapular stabilization plus thoracic extension work. Craniovertebral angle, neck pain, and disability improved in both the intervention and the control group (which did cervical stretching instead), so thoracic extension wasn't the secret sauce for posture per se. Where it did pull ahead was respiratory function. Maximum inspiratory pressure, maximum expiratory pressure, and forced vital capacity all improved significantly only in the thoracic extension group. That's interesting enough to keep the exercise in. A 2021 systematic review and meta-analysis (Jenkins et al.) confirms structured exercise reduces thoracic hyperkyphosis overall, though the evidence is rated low-to-moderate quality.
14. Cat-cow. On all fours, alternate arching and rounding. One vertebra at a time.
Research. Honest version: there's no RCT that isolates cat-cow and shows it does anything specific for posture. It comes from Stuart McGill's spine biomechanics work. His clinical case is that on all fours your body weight isn't loading the spine, so you're moving the segments through range with minimal compressive force, which McGill describes as the gentlest way to mobilize the spine. In his books he recommends around 5–8 cycles as a warm-up, not as therapy. The RCTs you'll see cited as "evidence for cat-cow" (like Ghorbani et al., 2018 showing pain and extension-ROM improvements at 6 weeks) are actually testing the McGill Big 3 (curl-up, side plank, bird dog). Cat-camel is the warm-up before those, not the intervention. So I'm keeping this as a low-risk mobility primer that a respected spine researcher recommends on biomechanical grounds, not because I have hard outcome data. Fine for that; I'd be lying if I said more.
Hips
15. Half-kneeling hip flexor stretch. One knee down, other foot forward, press the hips forward. One of the highest-impact stretches on this list for someone who sits all day.
Research. Most direct evidence I could find: a pre-post study on 23 men (Preece et al., 2021) measured pelvic tilt and passive hip extension before and after a single session of hip flexor stretching. They got a mean +2.6° in passive hip extension (P < .001) and a −1.2° reduction in anterior pelvic tilt (P < .001) in relaxed standing. No control group and the authors themselves note 1.2° on its own isn't clinically huge. But it's an acute change from a single session, and they cite prior work showing 6-week hip flexor stretching programs produce 13–15° gains in hip extension in people with real restriction. A 2024 crossover RCT on 26 active adults (González-de-la-Flor et al., 2024) tested the half-kneeling stretch with vs. without a posterior pelvic tilt cue and found the PPT version reduced reactive hip flexor force by 4.85 N·m (P = .003), meeting their threshold for clinical meaningfulness, without hurting hamstring flexibility. Translation: doing this stretch with your tailbone tucked under (glutes squeezed) is meaningfully better than just shoving your hips forward. I cue it that way.
16. Deep squat sit. Heels down, sit as low as you can, stay there. Opens hips and ankles that get locked from chair sitting.
Research. A 2020 PNAS paper by Raichlen et al. put accelerometers and EMG on Hadza hunter-gatherers and found that their "active rest" postures (full squatting and assisted squatting with heels on the ground) produced lower-limb muscle activity (soleus, vastus lateralis, tibialis anterior) around 20–40% of walking values, whereas chair sitting was close to baseline. Small biomechanical sample, specific population, so I'm not going to claim this fixes anything on its own. But it's good evidence that squatting is a fundamentally different muscular state than chair sitting, which is the main point. For the prerequisite question of whether you can deep squat, stepwise regression on squat depth (Kim et al., 2015) found ankle dorsiflexion and hip flexion ROM to be the main predictors in males (R² = 0.435), though in females ankle dorsiflexion plus dorsiflexor strength took over as the dominant predictors. So if your heels lift off the ground the second you drop down, the bottleneck is almost certainly ankles first.
Posterior chain
17. Prone YTW raises. Lie face down, arms form a Y (overhead), a T (horizontal), a W (elbows bent, arms pulled back). Strengthens the muscles between the shoulder blades that are supposed to hold posture up.
Research. Of everything on this list, this one has the deepest EMG literature behind it. The classic Ekstrom et al., 2003 EMG study (30 healthy subjects, 10 shoulder exercises) found that the prone overhead arm raise with external rotation (basically the Y-raise with thumbs up) produced 97% MVIC in the lower trapezius, the highest of any exercise tested, and also topped the list for middle trapezius along with prone horizontal extension with ER (the T). For the specific problem of restoring muscle balance (the right ratio of lower/middle trap to the overactive upper trap that tends to come with rounded-shoulder posture), Cools et al., 2007 (45 subjects, 12 exercises) identified four exercises with the lowest UT/LT and UT/MT ratios, including prone horizontal abduction with ER. Translation to outcomes in actual symptomatic people is weaker: a 6-week case series (not an RCT) in 40 overhead athletes with mild impingement (De Mey et al., 2012) used a similar scapular-focused exercise set and saw Shoulder Pain and Disability Index scores drop from 29.86 to 11.7 (P < .001). Uncontrolled design means that number has to be read with a grain of salt, but the direction lines up with the EMG work. I'm keeping this as the anchor strength exercise of the program.
18. Caterpillar walk (inchworm). Stand, fold forward, walk the hands out to a plank, walk them back. Moving plank that hits hamstrings, back, and shoulders at once.
Research. Nothing tests caterpillar walk directly. Its components have evidence, but indirect: core EMG during plank has been reviewed at scale (Oliva-Lozano & Muyor, 2020), and dynamic hamstring stretching acutely increases knee-extension ROM by 7–10% with the gain sustained for at least 90 minutes (Nakamura et al., 2017, n=24). The honest version: the inchworm passes through those two positions transiently rather than dwelling in either, so I can't promise you the same effect sizes. I keep it because it's a cheap way to hit the posterior chain dynamically in about 20 seconds, not because the research specifically validates it.
7. The whole plan
Not a 30-day challenge. Posture doesn't rebuild on a 30-day timer, and the research bears that out. Most of the RCTs I cite above ran 4 to 12 weeks at 3×/week as a minimum effective dose. I'm going longer. Day 30 is a milestone, not a finish line.
- Duration. At least 2 months. Could be all of 2026, or whatever's left of it.
- Dose. 5 minutes per session. 3 short sessions spread across the workday. A few sessions just to remind myself a few times per day about posture.
- Trigger. I'll use my own extension, 1 Pixel Workout, to interrupt me mid-doomscroll and drop me into a workout. Just need to add a pack of chosen exercises.
- Content rhythm. One short video per day. A qualitative check-in (video + journal note) every 2 weeks. A full measurement check-in video every 30 days, with the new numbers and a side-by-side photo.
- Journal. The full day-by-day log is at 📓 Posture Experiment Journal. That's where I record what I actually did, reps, hold times, and what I skipped.
- Primary success metric. Two of the four home measurements moving in the right direction over 90 days. I don't care which two.
- Secondary success metric. Not cringing at the next side-profile photo.
8. What I'm asking from you
The blog itself doesn't have comments (yet). But I want to hear from you. Two places work:
- YouTube comments under the video. That's where I'll be reading and replying the most.
- Email reply. If you're on the newsletter (form at the bottom of this page), just hit reply. It comes straight to me.
Two specific asks:
If you've actually fixed your posture or mobility, tell me what worked. Specific exercises. Specific dose. Specific results.
If something in this plan looks dumb to you, say that too. I'd rather get roasted now than spend a year on the wrong exercises. I'm not a professional. I'm guessing based on what two doctors told me, what the research supports, and what I could measure at home. All three inputs are fallible.
I'll read every comment and every email. The plan will evolve based on what makes sense.
9. What the research actually says
Pulled from the 130+ peer-reviewed studies that went into building this list. If you want a single paragraph to take with you:
Combined strengthening-and-stretching programs outperform single-modality approaches. The strongest direct evidence supports chin tucks (Level 1a, meta-analysis of 7 RCTs) for forward head posture, prone Y-T-W raises (97% MVIC activation) for lower trapezius recruitment, and doorway pec stretches (multiple RCTs) for rounded shoulder correction. The key dose-response finding: 4 to 12 weeks at 3×/week is the minimum effective dose for measurable postural change. The key nuance: stretching alone rarely changes posture long-term, but it restores the range of motion that makes strengthening work actually possible.
For thoracic kyphosis specifically, two meta-analyses (González-Gálvez et al., 2019; Jenkins et al., 2021) found structured exercise programs effective. González-Gálvez (10 RCTs, 539 participants) reported a large pooled effect (SMD = −1.40), with strengthening doing more of the work than stretching. Jenkins is more nuanced: large effects in younger adults (SMD = −2.8), much smaller in older adults (SMD = −0.3), and only programs of three months or less worked. Quality of evidence was rated low-to-moderate. For anterior pelvic tilt, the evidence is much weaker — Falk Brekke et al., 2020 found only four eligible studies (95 patients total) and graded the overall certainty as "Very low." A small adolescent study (Ludwig et al., 2016) reported a 3.3° APT reduction from combined strength + sensorimotor training versus 1.6° from strength alone, but it's adolescents, not adults, so applicability to desk workers is unclear. For forward head posture in office workers, Yaghoubitajani et al., 2022 — a small (n=36) RCT — found online-supervised delivery at least as effective as in-person workplace coaching. That matters for anyone trying to do this at their desk.
How long before I'll see changes? Honest answer: I don't know. Nobody does, not for an N=1 experiment with my specific mix of issues. The research averages suggest 4 to 12 weeks to move a measurement. My plan is to report the numbers every 30 days and let the data speak.
The full citation list is embedded above in each exercise section.
10. FAQ
What is osteochondrosis? Osteochondrosis is wear on the discs between your vertebrae. The discs lose water and elasticity, so they cushion the spine less well. Mild forms are common in adults over 30 and often cause no pain.
What is spondylosis? Spondylosis is age-related wear of the spine. The body grows small bony outgrowths called osteophytes to stabilize loose areas. Mild spondylosis is common after 40 and is usually symptom-free.
Can you reverse scoliosis with exercise? Mild scoliosis under 10 degrees is usually managed with exercise and monitoring. Exercise will not straighten the spine, but it can reduce pain and slow progression. Ask your doctor about your specific curve.
Where can I see what you actually did each day? The full day-by-day journal lives at 📓 Posture Experiment Journal. Each entry lists the exact exercises, hold times, and any skipped sessions.
How long does it take to fix forward head posture? Research on therapeutic exercise shows measurable improvement in 4 to 12 weeks of consistent work. Full correction often takes longer and depends on how long the pattern has been in place.
What happens next
Day 1 starts 18 of April 2026. First check-in video in 2 weeks with qualitative notes. First real measurement re-check at day 30.
The easiest way to follow along is the newsletter. Form is right below this post. Drop your email and I'll send you every check-in, every new number, and any course corrections I make. No spam. If I have nothing to say, I don't email.
You can also:
- Subscribe on 1 Pixel Workout Youtube channel and do some workouts too (I'm going to post shorts every day).
- Install 1 Pixel Workout and do the breaks with me.
If you don't, that's fine. I'm doing this either way.
↓ Newsletter form is right below. ↓
Cheers, Denys